
CT case study – Dog with chronic nasal discharge
Check out below: Dog with chronic nasal discharge
CT case study – Dog with chronic nasal discharge
History
A male neutered, 11yr 6-month flat coated retriever was presented with a 2- month history of left sided nasal discharge.
On clinical examination the patient was bright. There was muco-purulent nasal discharge from the left nostril however no obvious change in respiratory noise was present. There was mild-moderate periodontal disease affecting the oral cavity, but no other oral abnormalities were identified. The head and neck were palpably normal and there was no palpable regional lymphadenopathy. Thoracic auscultation and abdominal palpation were unremarkable, and the patient was normothermic. Direct auscultation over the laryngeal area revealed that there was a mild increase in inspiratory noise. Assessment of the displacement of a small piece of cotton wool held in front of each nostril revealed that the airflow through the right nostril was present, however no airflow was evident through the left nostril.
A space occupying lesion within the left nasal cavity was suspected and a computed tomographic (CT) study was undertaken using a GE Revolution ACT Scanner.
Computed tomography protocol
Under general anaesthesia the patient was positioned in sternal recumbency on the CT table, head first. The forelimbs were retracted, and the collar removed in order to avoid photon starvation, which can cause streaking artefacts. The scan was acquired using 1.25mm slice thickness, from the tip of the nose to the level of the 3rd cervical vertebra, thereby ensuring inclusion of the retropharyngeal lymph nodes.
The data produced from each CT scan can be processed using different reconstruction kernels or “filters” that optimise the image produced according to the tissue of interest. Soft tissue reconstructions increase contrast within soft tissue and reduce “noise” however the image is less sharp. Bone reconstructions are sharper and help to highlight changes within bone but introduce more “noise” reducing contrast. In most cases multiple reconstructions are always utilised because each provides complementary diagnostic information.
It is also important to perform contrast enhanced CT studies when soft tissue or organs are evaluated. By acquiring CT images before and after the intravenous administration of iodinated contrast media, the vascularity of tissue can be assessed, and some lesions are better or only visualised on post-contrast images.
For this patient both pre- and post- contrast images were acquired, and bone and soft tissue reconstructions were performed for both, respectively.
Findings
Image 1:

Axial pre-contrast soft tissue reconstruction image, the left side is denoted by the “L”. A large, isoattenuating (i.e. same grey-scale as the surrounding soft tissues) region occupies the entirety of the left caudal nasal passages (red arrowhead), consistent with a soft tissue mass or fluid accumulation.
Images 2 and 3:
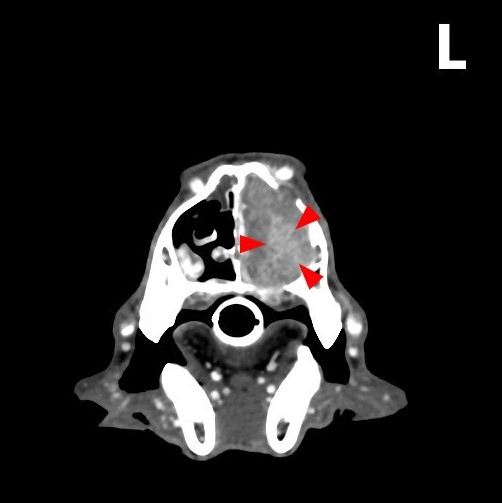
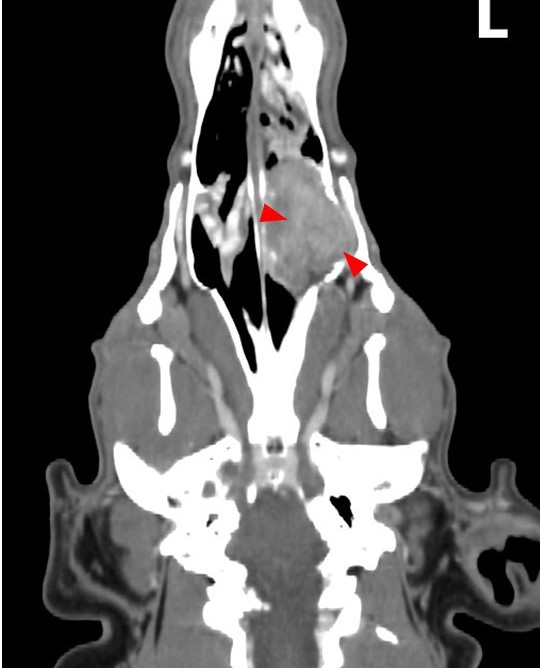
Axial post-contrast soft tissue reconstruction image (left) and a dorsal post-contrast soft tissue reconstruction image (right). There is contrast enhancement (increased attenuation [lighter grey] as a result of accumulation of contrast media, red arrowheads). This highlights the vascular perfusion of the pathology and confirms the presence of a soft tissue mass rather than fluid accumulation.
Image 4:
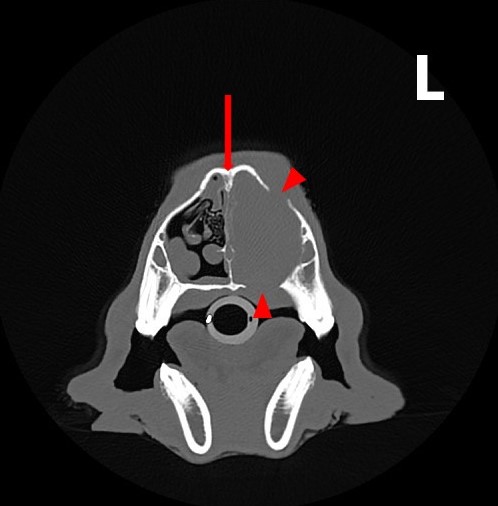
Axial pre-contrast bone reconstruction image at the level of the mass. There is marked destruction of the nasal turbinates compared with the right caudal nasal cavity. There are multiple areas of bone lysis around the mass (red arrowheads). The nasal septum is deviated to the right-hand side (red arrow). These findings also indicate the presence of a space occupying mass.
Image 5:
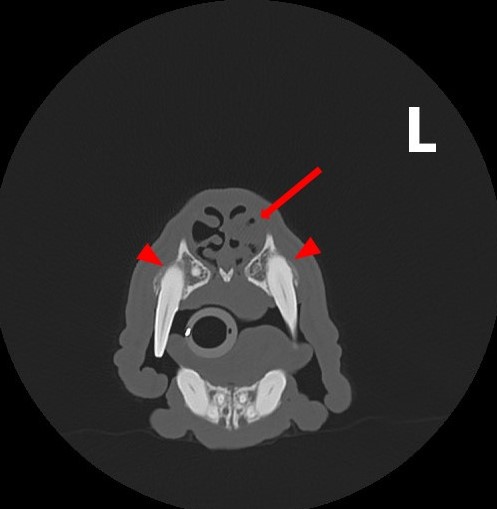
Axial pre-contrast bone reconstruction image at a level rostral to the mass. There is fluid accumulation and soft tissue thickening within the left nasal cavity (red arrow) and new bone formation at the alveolar processes of 104 and 204 (red arrowheads). The new bone formation around the canine teeth was considered to be secondary to chronic periodontal disease.
Image 6:
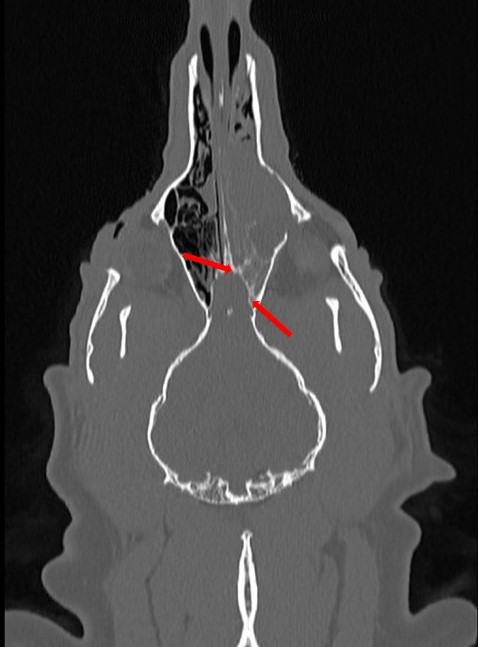
This pre-contrast bone reconstruction image is at the level of the cribriform plate (red arrows). The cribriform plate is part of the ethmoid bone and marks the boundary between the nasal cavities and the cranial cavity through which the olfactory nerves travel. In this case there is no obvious defect in the cribriform plate. Therefore, there is no evidence suggestive of neoplastic invasion of the cranial cavity, although it cannot be entirely ruled out from the images alone.
From the CT images it can be concluded that there is an aggressive soft tissue neoplasm within the caudal left nasal cavity. This has resulted in multifocal osteolysis and an obstructive frontal sinus effusion. There is also evidence of periodontal disease effecting the upper canine teeth.
Discussion
Nasal cavity tumours account for approximately 1% of all neoplasms in dogs1. Two thirds of nasal neoplasms are epithelial carcinomas (adenocarcinoma, squamous cell carcinoma) and one third are mesenchymal in origin (fibrosarcoma, chondrosarcoma or osteosarcoma)2. Nasal neoplasms tend to be locally invasive with low rates of metastasis.
Clinical signs associated with nasal neoplasia include:
- Nasal discharge
- Epistaxis
- Sneezing
- Stridor/stertor
- Facial deformity
- Epiphora
- Reduced airflow through the affected nostril
Computed tomography is ideal for evaluating and staging nasal neoplasia because superimposition of the complex nasal cavity anatomy is avoided. In addition, soft tissue versus fluid (such as mucus accumulations) can be distinguished, especially when contrast enhanced CT is used. Magnetic resonance imaging (MRI) can be similarly beneficial in nasal neoplasia cases, however the availability of MRI is much more limited.
Radiography can be used to evaluate the nasal cavity. Under general anaesthesia an open mouth dorsoventral view can be acquired to avoid superimposition of the mandible. For this view the plate is placed intraorally, and the beam directed from above. However, soft tissue versus fluid cannot always be easily distinguished, and superimposition of the complex anatomy can lead to missed lesions or information.
A complete blood count, serum biochemistry profile and clotting times should be assessed prior to biopsy techniques. Biopsy can be performed via rhinoscopy or using a blind technique using forceps via the nasal cavity. The latter technique is more applicable if the tumour is large and it is important to measure the length of the forceps to avoid damaging caudal nasal cavity structures such as the cribriform plate.
Radiotherapy is the treatment of choice for most nasal neoplasia cases3,4 though this is usually aimed at palliative care given the close nature of the brain and eyes.
References
- Malinowski C. (2006) Canine and Feline Nasal Neoplasia. Clinical Techniques in Small Animal Practice 21: 89-94.
- Forrest L. (2018) The Cranial Nasal Cavities: Canine and Feline, In: Textbook of Veterinary Diagnostic Radiology 7th edn., Ed: Thrall D., Elsevier, St. Louis, pp 183-203.
- Elliot K.M., Mayer M.N. (2009) Radiation therapy for tumors of the nasal cavity and paranasal sinuses in dogs. Canadian Veterinary Journal 50: 309-312.
- Woodruff M.J., Heading K.L., Bennett P. (2019) Canine intranasal tumours treated with alternating carboplatin and doxorubin in conjunction with oral piroxicam: 29 cases. Veterinary and Comparative Oncology 17: 42–48.
We hope you enjoyed this blog post: Dog with chronic nasal discharge
class=”yoast-text-mark”>style=”font-family: Arial, Helvetica, sans-serif;”>

Don’t forget to share! 👇