
Thoracic Radiology Case Study – Indoor cat with an acute subluxated xiphisternum
Check out this Thoracic Radiology Case Study below:
History
A 2-year-old male neutered domestic short-haired cat presented with acute onset tachypnoea and thoracic pain following an episode of fighting with another cat in the household. The owners reported feeling an abnormal protrusion on the ventral thorax that hadn’t been present previously. The cat had been in their possession since it was an 8 week old kitten.
On clinical examination, the patient was bright, alert and responsive. The mucous membranes were pink and moist, with a capillary refill time of one second. The heart rate was 184 beats/minute with no audible gallop rhythm present, and the respiratory rate was 104 breaths/minute with clear breath sounds and no adventitious lung sounds on auscultation. There was no open-mouthed breathing, but the cat was displaying a restrictive breathing pattern without abdominal effort. The patient was normothermic with a rectal temperature of 38.1°C. On examination the cat was reactive when lightly palpated over the mid to caudal thoracic vertebrae (T8-T13). No obvious rib fractures were detected. A non-mobile bony protrusion surrounded by a mild soft tissue swelling could be palpated ventral to the caudal aspect of the sternum, which measured approximately 1cm in width and 2cm in length. On palpating this region, the cat became notably distressed and uncomfortable.
The patient was given oxygen supplementation and intramuscular pain relief (0.2mg/kg bodyweight methadone – Comfortan© 10mg/ml solution; Dechra Veterinary Products) prior to further diagnostic investigation. The cat was negative for free fluid on Thoracic Focused Assessment with Sonography for Trauma (T-FAST) examination. The cat was transferred to a quiet ward and the respiratory rate reduced to 36 breaths/minute.
Thoracic Imaging
Once the patient was stabilized, a conscious dorsoventral survey radiograph was acquired to assess for disease affecting the thoracic cavity (Image 1). There was no radiographic evidence of pleural effusion, lower airway or parenchymal disease present. The margins of the heart were not clearly defined, however this was likely due to positioning and radiographic exposure being taken upon expiration. There were no obvious rib fractures present.
Once it was established that there were no imminently life-threatening conditions affecting the thorax, an orthogonal view was acquired (Image 2).
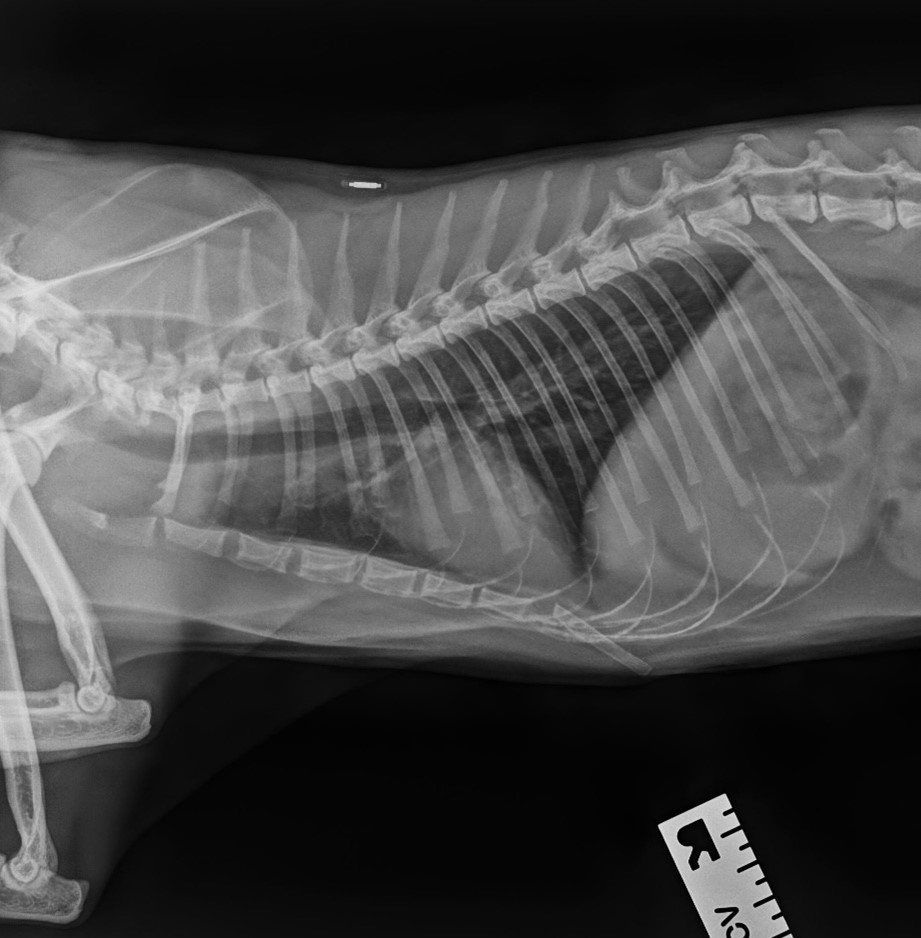
On the right lateral thoracic radiograph, there was subluxation at the articulation between the 7th sternebra and the xiphoid. The caudal aspect of the xiphoid deviated ventrally. The subluxated xiphoid did not appear to penetrate the ventral thoracic wall. The rest of the thoracic cavity, including the lung fields and the heart, appeared to be within normal limits. There was no evidence of a pneumothorax or subcutaneous emphysema in the region of the subluxation.
Findings
Image 1: Dorsoventral conscious survey radiograph of the thoracic cavity

Image 2: Right lateral radiograph of the thoracic cavity illustrating the subluxation at the articulation between the 7th sternebra and the xiphoid (white arrow)
Image 2: Right lateral thoracic radiograph.
Diagnosis: Traumatic subluxation of the articulation between the 7th sternebra and the xiphoid.
Possible differential diagnoses:
- Pectus excavatum – a congenital abnormality of the thoracic cavity. This condition is characterized by a prominent dorsal deviation of the caudal sternebrae resulting in an indentation of the junction between the caudoventral thoracic and the cranial abdominal walls 1.
- Flat-chested kitten syndrome (FCKS) – a thoracic angular deformity which is characterized by the flattening of the ribcage along its entire length. This results in a very flat sternum that can occasionally be dorsally deviated. Affected kittens have sharp lateral angulation of the costochondral cartilages affecting both the cranial and caudal ribs. A marked dip in the spine over the shoulder region is also commonly observed1.
Management and outcome
The patient was managed conservatively. Anti-inflammatory medication was used to manage the patient’s clinical signs and the owner was instructed to monitor for respiratory distress. The patient was discharged with oral meloxicam (Metacam Oral Suspension 0.5mg/ml; Boehringer Ingelheim Animal Health UK), to be given at a dose of 0.05mg/kg body weight every 24 hours for 7 days. The patient was re-examined at 2 and 14 days post discharge from the small animal hospital. On re-examination at day 2, the owners reported that although quieter than usual, the cat had returned to its normal routine and displayed no increase in respiratory effort or rate. On palpation of the subluxated xiphisternum, mild soft tissue swelling remained, along with increased sensitivity. When re-examined at day 14, the owners reported that the cat was continuing to do well and had returned to normal demeanor. There was improved comfort on palpation of the sternum and the soft tissue swelling had resolved. Due to the improvement, no further non-steroidal anti-inflammatory medication was deemed necessary, and the owners continued with conservative management at home through the monitoring of respiratory rate and effort. The patient was not re-examined again.
Discussion
Radiography plays an important role in confirming the diagnosis of thoracic disease. In cases of unstable patients, a point-of-care ultrasound is particularly useful to confirm the presence of pleural or pericardial effusion or air. When performing thoracic radiographs on patients presenting with dyspnoea, orthogonal views should only be attempted after the patient has been stabilised. The required views should include a ventrodorsal or dorsoventral and lateral thoracic radiographs.
With any possible thoracic injury, care should be taken when positioning the patient so as not to compromise respiration.
In feline anatomy, there are normally 8 sternebrae. The first is the manubrium, followed by 6 sternebrae which form the body of the sternum, and lastly the 8th sternebra, known as the xiphoid. The xiphoid is continuous caudally with the xiphoid cartilage; they are known together as the xiphisternum2. While 8 sternebrae are normal, congenital abnormalities causing alterations in the number of sternabrae are common and typically of no clinical significance3.
There are few reports in the literature regarding sternal luxation or subluxation in cats. Since trauma is reported as being the most common cause, it is possible that other concurrent life-threatening conditions resulted in the death or euthanasia of a patient before findings could be reported4.
From the four reported cases of cats with either sternal luxation or subluxation, both medical and surgical management has been described4–7. Lam (2018) describes a 1-year-old female neutered cat that was successfully managed conservatively following subluxation of the articulation between the 6th and 7th sternebrae4. Surgical management was reported by Choi, wherein two cases of sternal luxation (one patient with a 6-7th sternal luxation and one patient with a 4-5th sternal luxation) were successfully managed by either immediate or delayed surgical correction7. Despite these successful cases, a case report in 2015 describes a cat with a manubrio-sternal luxation and tracheal stenosis following a road traffic accident5. Despite surgery, the patient was euthanased intra-operatively due to dehiscence of the surgical site5.
In the textbook of Small Animal Surgery, in addition to comments that sternebral luxations are occasionally seen with thoracic trauma, a method of surgical repair via internal fixation using an orthopaedic wire and small intramedullary pins is described 8. In contrast to this, the textbook of Small Animal Surgical Emergencies describes a case report of a cat with a subluxation of the sternum at the articulation between the 5th and 6th sternebrae following a dog attack 6. In this case, the thoracic wall injuries were managed conservatively with intravenous fluid resuscitation, analgesia, oxygen supplementation and antimicrobial therapy 6. Despite complications due to a radius-ulna fracture, the cat improved and was discharged. Although most sources report that these cases present as a result of a traumatic incident, it is referenced in Feline Diagnostic Imaging that ventral deviation of the xiphoid can be a normal variation in cats 3.
There are similarities between the current patient and the case report from Lam (2018). Both cases were indoor cats presenting with tachypnea and a protrusion on the ventral thorax. In the Lam (2018) case, the radiographic diagnosis was subluxation of the articulation between the 6th and 7th sternebrae with slight deviation between the 7th sternebra and the xiphoid 4. As with the present case report, there was no penetration of the thoracic cavity by the bony protrusion and no evidence of ongoing dyspnoea, so a similar conservative management approach was implemented4. This strategy was further supported by the case report described in the Small Animal Surgical Emergencies textbook 6.
Similar to the few reported cases of sternal luxation or subluxation in cats, there are also few known cases in dogs. The first reported successful management of a traumatic sternal luxation in a dog was published in 2014 9, following only one previous report of a sternal fracture in 1985 10. In this case, the dog presented with dyspnoea, tachycardia and ventral thoracic discomfort following a fall down the stairs. Thoracic radiographs revealed a luxation between the 3rd and 4th sternebrae with dorsal displacement of the caudal segment 9. This case was surgically managed through reduction and stabilization of the luxation using a dynamic compression plate 9. Although this was successful, sternal reduction involves intra-thoracic surgery which carries potential complications.
Although not performed in the previous case, computed tomography (CT) is indicated if concurrent injury to the thoracic organs is suspected, such as in cases of traumatic luxation of the sternum 11.
In conclusion, the frequency of sternal luxations and subluxations in cats in veterinary practice is still unknown. As the reports in veterinary literature are rare, the proper management of these cases is open to discussion. Further reporting of similar cases is necessary to discover the true prevalence of this condition and the most appropriate treatment options.
- Charlesworth, T. (2017) Pectus excavatum: congenital thoracic deformity in cats. In Practice 39, 73–78.
- Coulson, A. and Lewis, N. (2008) Cat: Ribs & Sternum. In: An Atlas of Interpretative Radiographic Anatomy of the Dog & Cat, Blackwell Science Ltd, Oxford, UK. pp 480–483.
- Larson, M.M. (2020) Thoracic Cavity. In: Feline Diagnostic Imaging, Eds: M. Holland and J. Hudson, Wiley. pp 281–286.
- Lam, L. (2018) Acute sternal subluxation in an indoor cat. The Canadian veterinary journal = La revue veterinaire canadienne 59, 82–84.
- Pietra, M., Pisoni, L., Linta, N., Pinna, S., Romagnoli, N. and Diana, A. (2016) Endoscopy-assisted tracheal reconstruction of post-traumatic obstruction in a cat: a case report. Veterinární Medicína 60, 341–344.
- Savini, J. and Silverstein, D. (2015) Chest Wall Disease: Stabilization Techniques for Patients with Chest Wall Disease. In: Small Animal Surgical Emergencies, Ed: L.R. Aronson, John Wiley & Sons, Inc., Chichester, UK. pp 350–354.
- Choi, G.C., Rahman, M.M., Kim, H., Kim, S. and Jeong, I.S. (2018) Management of sternal dislocation with and without surgery in cats: Owner-assessed long-term follow-up of two clinical cases. The Journal of veterinary medical science 80, 1001–1006.
- Orton, C.E. (2002) Thoracic Wall. In: Textbook of Small Animal Surgery, 3rd ed., Ed: D. Slatter, Saunders, Philadelphia . pp 382–383.
- Serra, C.I., Soler, C., Moratalla, V., Sifre, V. and Redondo, J.I. (2015) Surgical management of a traumatic dislocation of the sternum in an English bulldog. The Journal of small animal practice 56, 407–10.
- Newton, C.D. (1985) Fractures of small bones. In: Textbook of Small Animal Orthopaedics, Eds: C.D. Newton and D.M. Nunamaker, JB Lippincott, Philadelphia, PA, USA. pp 325–329.
- Velissaris, T., Tang, A.T.M., Patel, A., Khallifa, K. and Weeden, D.F. (2003) Traumatic sternal fracture: outcome following admission to a Thoracic Surgical Unit. Injury 34, 924–927.
We hope you enjoyed this blog post!
Don’t forget to share! 👇