Small animal veterinary case study – Amber the domestic shorthair
Case provided by Yvonne McGrotty BVMS CertSAM DipECVIM-CA MRCVS
European Specialist in Veterinary Internal Medicine
RCVS Specialist in Veterinary Internal Medicine
History:
Amber is a 12yr FN DSH. She was presented with a 4-month history of vomiting. Vomiting occurred once or twice daily and consisted of a mixture of food and fluid. Occasional diarrhoea was also reported but this was infrequent. Appetite was good but there had been some weight loss. The cat was reported to be somewhat less active.
Physical Examination:
On clinical exam Amber was quiet but responsive and in good body condition at 3.8kg. Mucous membranes were pink and moist and CRT was less than 2 seconds. Thoracic auscultation was unremarkable. On abdominal palpation organomegaly was detected, thought to be a thickened stomach.
Haematology and biochemistry were unremarkable and TT4 was within normal limits.
Diagnostic Imaging:
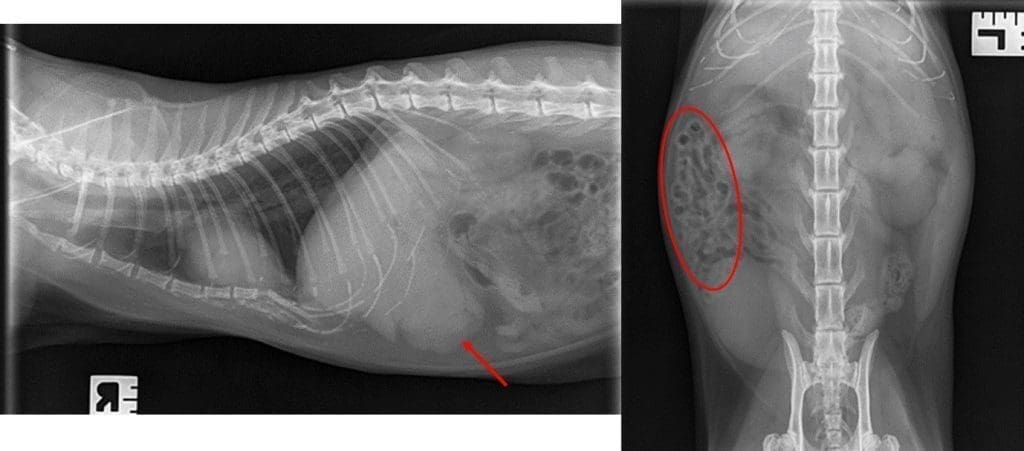
Excellent quality survey radiographs were obtained by the referring vet. These showed a soft tissue density in the cranioventral abdomen caudal to the liver (Figure 1). Small intestinal loops were displaced to the right. The lateral thoracic radiograph was mostly unremarkable with no evidence of pulmonary parenchymal disease.
Figure 1. A right lateral thoracic X-ray showing part of the cranial abdomen (Left) and a dorsoventral abdominal X-ray (Right). A soft tissue density mass is visible in the cranioventral abdomen (red arrow) and the small intestine is displaced to the right abdomen (red circle).
Abdominal ultrasound confirmed that the gastric wall was markedly thickened and had lost its normal layering (Figure 2). Wall thickness was around 1.39cm for approximately 50% of the body of the stomach. Two local lymph nodes, including the gastrosplenic lymph node, were enlarged and hypoechoic. The remainder of the scan was unremarkable.
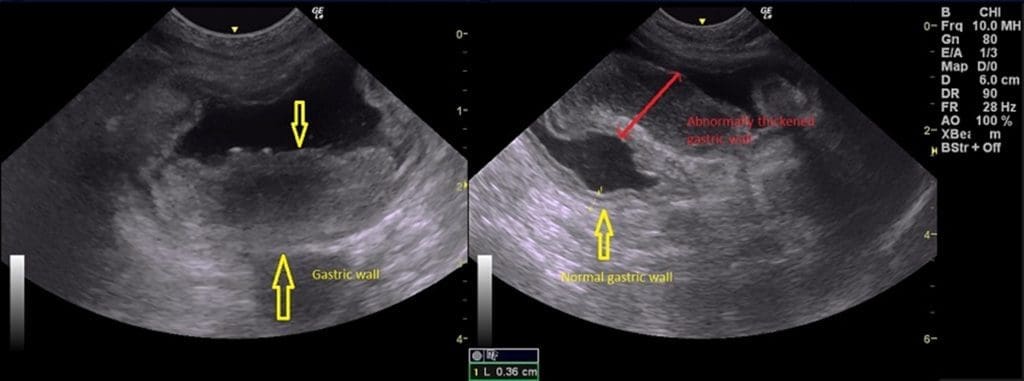
Figure 2. Two ultrasound images showing a transverse section of the stomach. In the left image a markedly thickened gastric wall with loss of normal layering can be seen (between yellow arrow). In the right image a similarly altered section of the wall is visible (red double-headed arrow), however, a section of gastric wall with a normal thickness and layered appearance is visible (yellow arrow).
Differential Diagnosis:
- Gastric lymphoma
- Gastric adenocarcinoma
- Inflammatory bowel disease
Further Investigations:
Further investigations could include ultrasound guided FNAs of the thickened gastric wall and enlarged lymph nodes, biopsies of the gastric wall using endoscopy or exploratory surgery with biopsy of the gastric wall and lymph nodes. FeLV and FIV testing would also be appropriate. In this case the cat was negative for both FeLV and FIV.
Gastroscopy was performed. The oesophagus was unremarkable. The stomach was markedly abnormal with an irregular appearance. The rugal folds were thickened and had prominent light reflectivity which may suggest oedema. Ulceration was not present. The mucosa was very friable and easy to biopsy. The duodenum was examined and the mucosa was fairly unremarkable. Multiple biopsies were collected from the stomach which confirmed the presence of large lymphoid cells (Figure 3) consistent with gastric lymphoma.
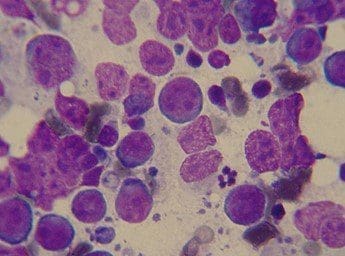
Figure 3. A photograph showing an impression smear from the gastric biopsies. A population of large lymphoid cells is visible with open chromatin, multiple nucleoli and scant basophilic cytoplasm consistent with lymphoma.
Treatment Options:
The tumour is unlikely to be confined to the stomach so surgical removal is unlikely to be of benefit especially since local lymph nodes were enlarged. In addition, the area of stomach involved was considerable. Steroids alone would provide short term palliation. Chemotherapy would be the most effective form of therapy, however duration of remission with COP-based protocols would still be relatively short. More extensive chemo protocols could be considered.