Emergency abdominal ultrasound in equine practice
An in-depth description of the steps required to carry out an emergency abdominal ultrasound using the FAST scanning technique.
Background
FAST (Focused Assessment with Sonography for Trauma) scanning is now a routine diagnostic tool in human trauma medicine for detecting the presence (or absence) of free abdominal fluid following blunt abdominal trauma. A modified form of this protocol has also become commonplace in small animal practice. More recently a system has been described (Busoni et al., 2011), based on these FAST protocols, for assessing horses with colic. This FLASH (Fast Localised Abdominal Sonography of Horses) protocol can be learnt easily and quickly by inexperienced operators and, as the name suggests, is performed rapidly in emergency situations to provide useful additional information required in the decision-making process when faced with a horse displaying symptoms of colic.
Preparation
Sedate the horse if necessary (though this is rarely required solely for the examination – sedation to control the pain associated with colic is more commonly the inciting reason for sedation in these cases).
Apply liberal quantities of surgical spirit/alcohol to the areas to be scanned. N.B. This can damage the latex covering on the end of the transducer – be sure to clean the probe afterwards using damp cotton wool. Remember that drips of alcohol running down the horse’s abdominal wall can cause them to fidget so wiping off excess spirit is wise.
Where possible dim the lights for the duration of the exam (although this is often not possible as frequently in the emergency situation the FLASH scan will be carried out simultaneously with other procedures, such as blood sampling, rectal examination etc.
Be sure to load patient details into the ultrasound machine before you start (where the clinical symptoms permit) to enable recording of images for the clinical records.
Technique
The protocol as described by Busoni et al. (2011) splits the abdomen into 7 ultrasonographic ‘windows’: ventral abdomen, gastric, spleno-renal, left middle third of the abdomen, duodenal, right middle third of the abdomen, and cranioventral thoracic (on the right side). These locations represent anatomical regions where pathology is mostly likely to be detected based on previous research.
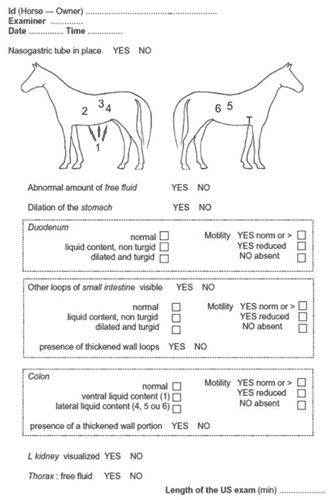
Using a low-frequency curvilinear (convex) transducer start at the ventral abdominal window on the ventral midline, moving through the ‘windows’ in sequence as listed above. At each site note the presence or absence of free abdominal fluid (visible as anechoic – black – regions, often triangular, between the abdominal viscera), the appearance of small intestinal loops, including their motility (or lack thereof), the contents of the large bowel, and the presence of the spleen in direct contact with the left kidney (at the spleno-renal window).
Interpretation
First and foremost this technique is used to detect the presence of free abdominal fluid, which is most frequently observed ventrally. Note that in horses a small amount of free abdominal fluid is considered normal, and the decision as to whether or not the amount of free fluid visible is increased above what would be considered normal is a subjective one. Also be aware that the nature of free abdominal fluid cannot accurately be assessed ultrasonographically – abdominocentesis and laboratory analysis of the fluid is necessary in these cases.
Small intestinal loops should be checked for degree of dilation, the presence or absence of turgidity, and motility. In their 2011 paper Busoni et al. found the presence of dilated, turgid small intestinal loops to have a sensitivity of 80% and specificity of 96.15% (positive predictive value 88.89%, negative predictive value 92.59%) for small intestinal obstruction.
A suspicion of nephrosplenic entrapment can be investigated using this protocol (via the spleno-renal window) – the presence of a gas-filled colon adjacent to the spleen, and an inability to visualize the left kidney support this diagnosis, though pairing this information with rectal palpation findings is wise (Scharner et al., 2002).
The Busoni et al. (2011) study did not investigate large colon wall thickness, but it has been shown that such measurements are useful in predicting large colon torsion (Pease et al., 2004) and can be made using this protocol.
Summary
The FLASH protocol is rapidly becoming a popular addition to the colic workup in many equine hospitals and is a useful technique for any equine veterinary surgeon to perfect. It can be learnt quickly, even if the operator is relatively inexperienced in the use of ultrasonography. Typically the entire exam takes little more than 10 minutes and can yield valuable information for decision-making in what can be very challenging circumstances. As with all diagnostic tools, it is important to remember that it represents but one piece of the jigsaw, so it should not replace a thorough approach to the rest of the examination.
References
Busoni, V., Busscher, V., Lopez, D., Verwilghen, D. and Cassart, D. (2011). Evaluation of a protocol for fast localised abdominal sonography of horses (FLASH) admitted for colic. The Veterinary Journal, 188(1), pp.77-82.
Pease, A.P., Scrivani, P.V., Erb, H.N., Cook, V.L. (2004). Accuracy of increased large-intestinal wall thickness during ultrasonography for diagnosing large-colon torsion in 42 horses. Veterinary Radiology and Ultrasound, 45, pp. 220-224.
Scharner, D., Rötting, A., Gerlach, K., Rasch, K. and Freeman, D. (2002). Ultrasonography of the abdomen in the horse with colic. Clinical Techniques in Equine Practice, 1(3), pp.118-124.
