Small animal veterinary case study – Sholto
Main body
Sholto was presented with a 4 month history of faecal tenesmus and haematochezia. The owner reported both fresh blood and melaenic stools. Some faecal mucus was also reported consistent with other signs of predominantly large intestinal disease. Initially signs had been intermittent but they were now a daily occurrence and Sholto had lost weight more recently. Faeces were now of cowpat consistency and faecal accidents were reported on a nightly basis. Appetite was stable and thirst was not increased. Vomiting was not a feature. Sulphasalzine therapy had proven ineffectual.
Haematology revealed severe thrombocytopenia. PT and APTT were within reference intervals and basal cortisol was within range, excluding hypoadrenocorticism. Faecal analysis and TLI, folate and cobalamin were unremarkable.
Physical examination
On clinical examination Sholto was bright and alert and in poor body condition at 23.5kg. Mucous membranes were pink and moist and there was no evidence of petechiation on the buccal mucosae. Thoracic auscultation was unremarkable and there was no evidence of pain on abdominal palpation. Rectal examination was performed; no masses were palpable and there was no blood in the rectum. Ecchymotic haemorrhages were identified on the left flank (pic). Systolic blood pressure was repeatedly found to be markedly increased (220mmHg).
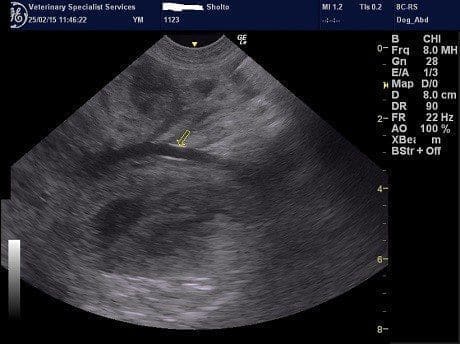

The transverse colonic wall was markedly thickened (>1cm) (pic). A large mass with irregular borders and mixed echogenicity was identified in the mid dorsal abdomen (pic). This mass was situated just cranial to the kidneys. The mass was well supplied with blood vessels, some of which were very large (pic). The mass was closely approximated with the abnormal piece of transverse colon. The origin of this mass was not identified on ultrasound due to its size so advanced imaging using MRI was performed.
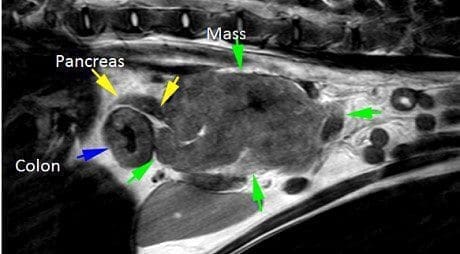
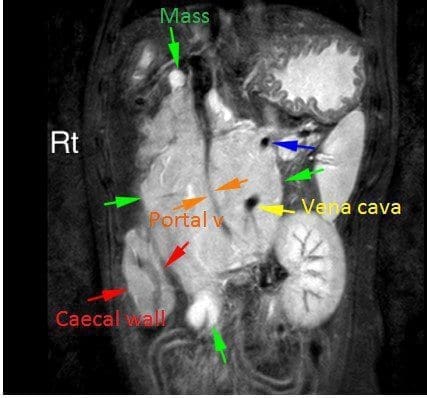
The MRI confirmed a multilobular irregular shaped mass in the cranial abdomen, which measures16cm (craniocaudal) x 6.9 cm (dorsoventral) x 8.0 cm (transverse). The mass surrounds the portal vein and branches of the portal system, the cranial mesenteric artery, and is resulting in a severe regional mass effect. The mass has a broad region of contact with the celiac artery, the distal ileum (at the level of the ileocolic junction), the caudal vena cava, and the ascending and transverse colon. At the level of contact with the colon, there is marked circumferential wall thickening, measuring up to 8 mm thick. There is also moderate diffuse thickening of the caecum. The margins of the pancreatic body and left pancreatic limb are in contact with this mass. Within the mid- to caudal aspect of the mass, there is marked narrowing of the portal vein and caudal vena cava. The jejunal lymph nodes are not seen. Multiple tortuous vessels are present along the periphery of the mass, most notable along the caudoventral margin. The pancreaticoduodenal vein is markedly tortuous, and subjectively enlarged, with a normal termination of the gastroduodenal vein into the portal vein. The right and left kidneys are moderately asymmetric, measuring 5.6 cm and 7.8 cm, respectively. The right kidney maintains a normal shape and similar signal intensity to the left. The adrenal glands are seen and unremarkable.
Diagnosis: Inoperable mesenteric mass involving major vessels and intestine
Large, extensive, mesenteric mass, with involvement of the ileocolic junction, transverse
colon, and perivascular involvement of the portal vein, caudal vena cava, and cranial
mesenteric artery. Organs of origin include colon/ileum, mesenteric, or lymph node (pancreas is possible).
There is evidence of collateral portal-portal venous shunting. The colonic and caecal wall thickening may be secondary to lesion extension, or regional oedema, inflammation, or haemorrhage. The T2 and STIR hyperintensity within the mass may represent necrosis, haemorrhage, or lymph.
Prognosis is extremely guarded as the mass is considered to be inoperable. Medical treatment has been started to hopefully raise Sholto’s platelet count which should reduce the risk of ongoing bleeding and make Sholto more comfortable.